2 Greenwich Office Park
Suite 210
Greenwich, CT 06831
203 863-0003
77 Lafayette Place
Suite 302
Greenwich, CT 06830
203 863-0003
21 Reade Place
Suite 2100
Poughkeepsie, NY 12601
203 863-0003
© 2024 The Plastic & Reconstructive Surgery Group - All Rights Reserved - Featured Realself Breast Reconstruction Expert - Terms of Use - Sitemap
One-Step Breast Reconstruction with Implants
Menu

One-Step Breast Reconstruction with Implants
Prepectoral Implant Reconstruction
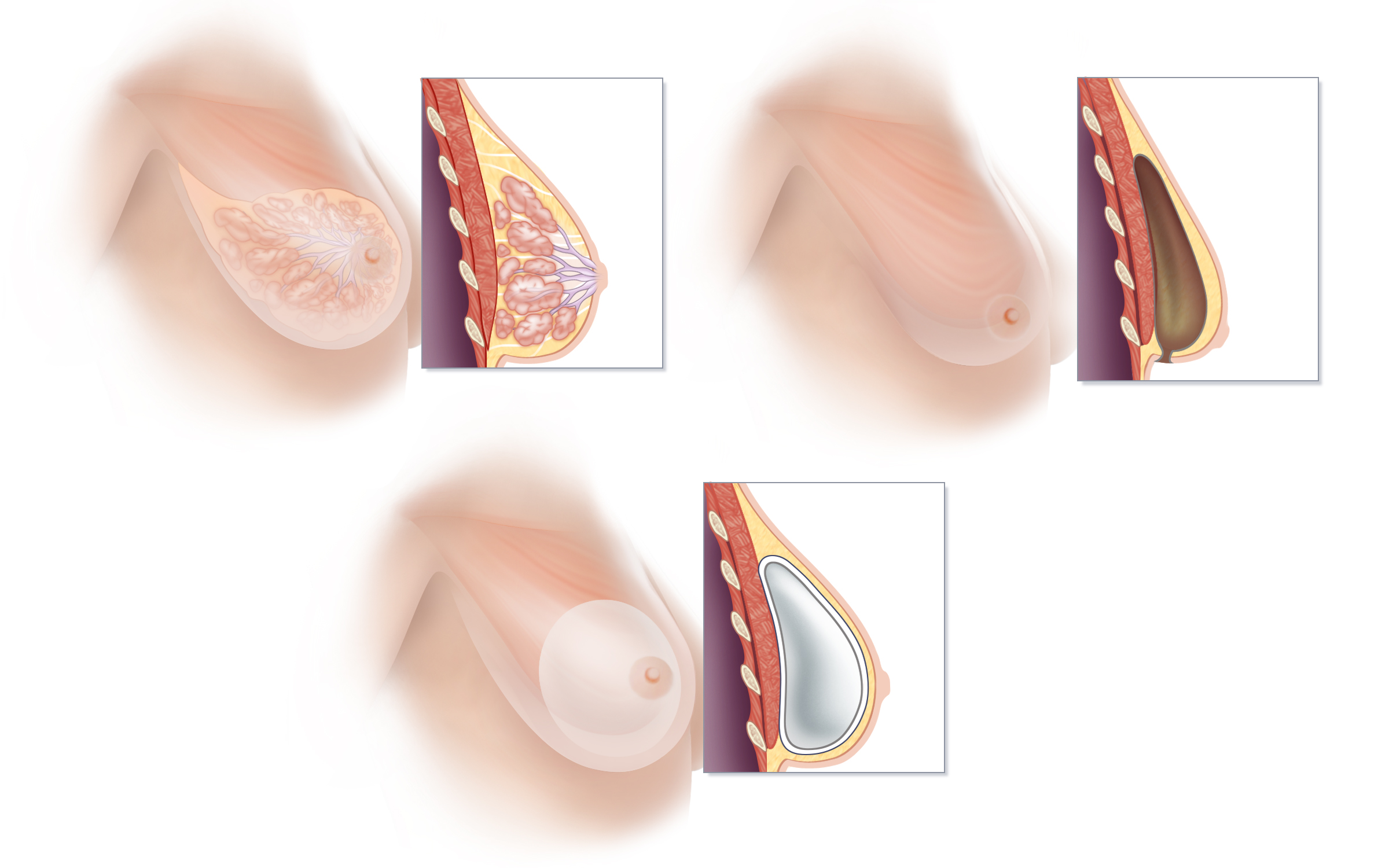
Prepectoral breast implant reconstruction is the current state-of-the-art method of implant-based breast reconstruction. This technique places an implant directly into the same space in which breast tissue is located prior to mastectomy. (A) Breast tissue is located on top of the muscles of the chest, between the pectoralis muscle and the skin. The lobules of the breast drain into a system of ducts that ultimately emerge through the nipple. (B) A mastectomy removes the tissue of the breast, and in so doing, inherently creates an empty space between the pectoralis muscle and the breast skin. (C) Prepectoral breast reconstruction restores the shape of the breast using an implant placed directly into the empty space created by mastectomy. Without disturbing the pectoralis muscle, a silicone-filled implant wrapped in specialized material known as acellular dermal matrix is inserted immediately following mastectomy. Prepectoral reconstruction avoids the weakness, discomfort, and visible movement of implants that can occur with muscle contraction (known as “animation deformity”) that commonly occur following traditional “under the muscle” implant (should this be implant-based) breast reconstruction.
Prepectoral breast implant reconstruction is the current state-of-the-art method of implant-based breast reconstruction. This technique places an implant directly into the same space in which breast tissue is located prior to mastectomy. (A) Breast tissue is located on top of the muscles of the chest, between the pectoralis muscle and the skin. The lobules of the breast drain into a system of ducts that ultimately emerge through the nipple. (B) A mastectomy removes the tissue of the breast, and in so doing, inherently creates an empty space between the pectoralis muscle and the breast skin. (C) Prepectoral breast reconstruction restores the shape of the breast using an implant placed directly into the empty space created by mastectomy. Without disturbing the pectoralis muscle, a silicone-filled implant wrapped in specialized material known as acellular dermal matrix is inserted immediately following mastectomy. Prepectoral reconstruction avoids the weakness, discomfort, and visible movement of implants that can occur with muscle contraction (known as “animation deformity”) that commonly occur following traditional “under the muscle” implant (should this be implant-based) breast reconstruction.
When used for breast reconstruction, breast implants can be placed on top of the pectoralis major muscle, using a technique called “pre-pectoral breast reconstruction” or under the pectoralis major muscle using the traditional “submuscular” approach.
Traditionally, women who have undergone implant reconstruction following mastectomy have initially had a tissue expander placed under the pectoralis chest muscle. Following an expansion process that requires regular visits to the surgeon’s office (in order to stretch the pectoralis muscle and create ample room for a breast implant of the desired size), a second surgery is done to remove the tissue expander and exchange it for a breast implant.
Our surgeons are part of group of innovative plastic surgeons who challenge the idea that implants must always be placed under the pectoralis muscle. To us, it simply makes the most sense, whenever possible, to replace volume directly where it is missing—right in the space that is left following mastectomy—rather than disrupt important and sizeable muscles, such as the pectoralis major muscle. This approach is favored in many cases because it is the philosophy of our team, regardless of the type of reconstruction we are performing, to preserve as much of a woman’s natural anatomy as possible, and to minimize interference with muscle function, strength and motion.
In comparison to techniques that place an implant under the pectoralis muscle, the placement of an implant in front of the pectoralis muscle means less pain, quicker recovery, less chronic discomfort or fatigue and less disruption of function. Furthermore, implants placed on top of the muscle do not flex or become distorted with pectoralis muscle flexion, upper body movements or exercise. Therefore, the unnatural movement and distortion of implants that is commonly seen when “under-the-muscle” implant reconstruction patients are moving their upper bodies or exercising (known as “muscle flex deformity” or “dynamic distortion”) is avoided. In fact, we sometimes relocate implants from below to above the muscle for women who are troubled by muscle-flex deformities.
Pre-pectoral implant reconstruction and traditional “behind the muscle” implant reconstructions each have certain advantages and disadvantages, so selecting which approach to recommend is done on a case by case basis.
The type of reconstruction you ultimately select should take into account the cancer treatment you require, your body type, your lifestyle, and your own goals for reconstruction. The risks and benefits of each type of breast reconstruction will be explored in detail at the time of your consultation.